
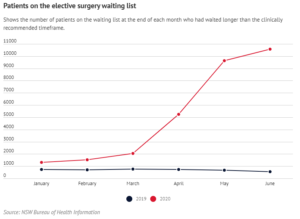
Elective surgery waiting lists continue to feature prominently in the headlines. In October, reports in the media said hospital waiting lists had skyrocketed by up to 40% as a result of a ban on surgery during the initial stage of the pandemic.
By June, there were more than 260,000 people waiting for elective surgery in Australia’s public hospitals, with those needing cataract surgery, hip and knee replacements and tonsillectomies facing some of the longest waits.
In an article in the Herald Sun, industry analyst Andrew Goodsall reported that a further 280,000 surgeries were estimated to have been deferred in the private sector, and said he predicts it will take almost two years to address the pre-pandemic backlog.
As well as delays caused by bans, other effects of the pandemic have included capacity issues due to social distancing, and appointments being cancelled for fear of contracting Covid19. Some people have also moved away from private insurance, adding pressure on the public healthcare sector.
Arguably attributable to declining private health insurance participation rates, combined with the ageing demographic, waiting lists were already at record high in many states by the time state governments imposed surgery bans to cope with the Covid-19 pandemic; in 2018-19 more patients were added to the public hospital elective surgery waitlist than were admitted for surgery.
While on the surface the decision to delay many types of non-urgent surgery in preparation for an influx of Covid-19 admissions made sense, and meant Australian hospitals coped remarkably well with the pandemic, it has left a legacy in the form of substantially inflated waiting lists. This has the potential to lead to a range of other health consequences.
The impact of deferred referrals
One issue that shouldn’t be overlooked is that of deferred referrals. During the pandemic, far fewer people have been presenting with symptoms or seeking primary and emergency care.
For example, cancer specialists have warned a hidden backlog of undiagnosed cancer cases are about to hit the health system after the number of breast cancer diagnoses fell by 37% in the first six months of this year.
To get on the waiting list, you first need to be seen by a consultant, and waiting times can be long for an appointment in public hospitals. It’s been reported that at some hospitals in South Australia, the wait for an appointment is years, with some people having waited more than a decade to see a specialist.
Available data doesn’t reflect a proportionate increase that might indicate that these missing referrals have started to come onto the list, yet. This hidden backlog is worrying, and may impact the waiting lists in other ways, since it may mean that by the time these people seek care, their condition may have worsened and they need more urgent care.
Although seen as non-urgent, many conditions are causing high levels of discomfort or disadvantage for patients, such as those who have waited a long time for cataract surgery, hip and knee replacements and tonsillectomies.
How bad is the situation?
 In June, waiting lists surged by 20% in NSW and by 40% in Victoria – before the second lot of restrictions – with a sizable waiting list also seen in other states. In Queensland, no new figures have been released on the size of elective surgery waiting list since the start of the pandemic, indicating there is an issue.
In June, waiting lists surged by 20% in NSW and by 40% in Victoria – before the second lot of restrictions – with a sizable waiting list also seen in other states. In Queensland, no new figures have been released on the size of elective surgery waiting list since the start of the pandemic, indicating there is an issue.
While urgent surgery has been going ahead, activity has been very low for some types of operations. As an example, the 50th centile waiting times for cataract extractions in Victoria has increased from 41 days in June 2019, to 262 days in June this year, while total hip reconstruction waiting times have seen a similar increase from 79 days in June 2019, to 292 days in June 2020, according to the latest figures from the Victorian Agency for Health Information.
In Victoria, capacity was subsequently heavily impacted by a second wave of Coronavirus when hospitals had to shut operating theatres, and the latest data reveals two out of three non-urgent operations had to be postponed between July and September. Although the situation with Covid-19 is looking better and elective surgery activity has increased over the last few of months in Melbourne, clearing the backlog will take time.
Meanwhile the elective surgery list in NSW, where normal surgery activity levels have been maintained since 1 July, after falling by 40% between April and June compared to last year, has blown out to more than 100,000 patients. That’s a 20% increase, representing the largest jump in at least a decade.
In Queensland, a slowdown in elective surgery has also caused waiting lists to rise, as all but urgent surgery was suspended for about three months , with the so-called ‘wait list for the wait list’ particularly impacted. The state government has released figures showing there were 52,240 on surgery wait lists across Queensland on June 1.
But of course, June is some time ago now, and the question is what has happened to waiting lists since then.
Catching up with the backlog
A number of announcements with regards to funding have been made. For example, the NSW government has allocated $388 million for elective surgery catch up, while Queensland has pledged $250 million and the ACT $30 million to tackle the backlog. While the funding will help, the key issue is capacity; in terms of available theatre time, facilities, and surgeons being available for work.
Victorian Health Minister Martin Foley has suggested an elective surgery blitz to address waiting times will take place “as soon as it’s safe to do so”, and has called the Victorian health system “well-prepared, adaptable and resilient”. However, official figures show that there was a 52% drop in category 2 surgeries, and 77% drop in category 3 surgeries during July-September compared to the same period last year, indicating a low level of resilience.
The NSW branch of the Royal Australasian College of Surgeons said surgeons were now operating at more than 100 per cent capacity to clear the backlog, and should keep going through the Christmas break, especially in country towns with lower staff numbers and higher backlogs. There are also calls to recruit more nurses to help deal with the backlog.
In Tasmania, where elective surgery waiting lists were described as ‘at an all time high’ before Covid restrictions, the state government has pledged to invest an additional $45.5 million into elective surgeries over the next 18 months, in an effort to boost capacity.
But regardless of the financial situation, questions remain about how the promised extra 120 procedures a week can be delivered in practice, with hospitals already operating at or beyond capacity. Any funding announcements to ‘blitz’ waiting lists are also unlikely to have an impact on the hidden waiting list of patients who haven’t yet been able to get a first consultation with a specialist.
While private capacity can be used, the private sector is facing a backlog of its own and the sector was also affected by the restrictions on elective surgery in Victoria, due to a second outbreak in the spring.
Private Healthcare Australia CEO Rachel David recently said in an article that private hospitals were working overtime to clear their backlog, with up to 125% capacity achieved at times for routine surgery such as joint replacements, helped by the fact that private hospitals don’t have restrictions on the hours that operating theatres are open.
A resilient healthcare system
Although the Australian healthcare system managed the pressures of Covid-19 relatively well, the frequent claims about its resilience can be questioned. Is cancelling all routine activity to cope with a potential temporary spike in demand – or even limiting it to 75% of capacity – a sign of resilience?
While the current situation with Covid-19 is exceptional, it is also having lasting effects on the wider healthcare system, not least in terms of a backlog for elective surgery. Though classed as elective, some of the conditions can be painful and living with them for an extended period can have a severe impact on patients’ lives.
A resilient healthcare system has to have the flexibility to cope with temporary demand spikes and unforeseen emergency situations, within reason. But achieving such flexibility is not always easy; with limited capital budgets, space limitations within existing hospital buildings, and planning processes for both newbuild and redevelopment project taking many years, it can take time to build resilience.
 As a result, some providers have turned to temporary solutions such as prefabricated modular units or mobile clinical facilities, which can be deployed rapidly to extend a hospital’s capacity. Several Australian hospitals are already using flexible infrastructure to provide either replacement capacity while remodelling or refurbishing the existing department, or to boost surgical and diagnostic capacity in a bid to work through waiting lists much quicker.
As a result, some providers have turned to temporary solutions such as prefabricated modular units or mobile clinical facilities, which can be deployed rapidly to extend a hospital’s capacity. Several Australian hospitals are already using flexible infrastructure to provide either replacement capacity while remodelling or refurbishing the existing department, or to boost surgical and diagnostic capacity in a bid to work through waiting lists much quicker.
With flexible healthcare there is no need to wait for years for a new facility, or to cancel or postpone elective surgery to free up capacity on a temporary basis.
Preparing for the next pandemic
Mobile or temporary modular units should be seen as an extension of a hospital’s permanent facilities team, and as key to surge planning within the estate. The benefits are many. Such a solution could be used to expand either urgent or elective treatment capacity, or both. A mobile or modular healthcare facility can be rapidly repurposed to accommodate sudden changes of use, whether that is adding bed spaces or providing additional theatre, treatment or diagnostic capacity.
For example, a temporary ward could be converted into a level one respiratory support ward, while mobile operating theatres have the potential to be repurposed as HDU or ITU wards or to be used for procedures and treatments that benefit from the additional isolation, should another pandemic hit.
By default, these self-contained units tend to have separate entrance and exit points that don’t require the transportation of infected patients through other areas of the hospital. But they are equally suitable for providing a ‘cold’ zone to proceed with surgery without infection risk.
Although health services and providers are busy dealing with the current pandemic, it’s clear that there is a general need to increase resilience and the ability to adapt to changing demand in the long term. Waiting until the next wave of Covid-19, if it arises, or until a new pandemic could result in losing valuable time and delays in the implementation of suitable solutions.
Mobile and modular infrastructure can be deployed very quickly to help hospitals clear the inevitable backlogs in surgery, diagnostics and other procedures that have been postponed during the crisis.




