
Figures have repeatedly shown that the usage of diagnostic services aimed at detecting cancer is relatively lower among indigenous communities across Australia. Offering diagnostic procedures closer to patients, potentially outside a city hospital setting, could encourage uptake and allow more cancers to be detected early.
There is a correlation between remoteness and access to health services in general, but the picture differs between states and territories, and the matter of indigenous health is complex; demographics, socioeconomic status, culture, education, location and relative remoteness all play a part.
But regardless of location, Indigenous Australians are underrepresented when it comes to screening and diagnostic procedures aimed at detecting cancer, and this is a factor in the lower cancer survival rates seen in the Aboriginal and Torres Strait Islander populations.
Cancer outcomes
According to projections based on the 2016 Census of Population and Housing, around 864,200 people identified as Indigenous Australians in 2020. There are hundreds of individual groups, each with its own distinct language, history and cultural traditions. Although an estimated 62% of Aboriginal and Torres Strait Islander population in Australia live outside major cities – and account for a high share of the population living in remote areas – most live in urban or regional areas.
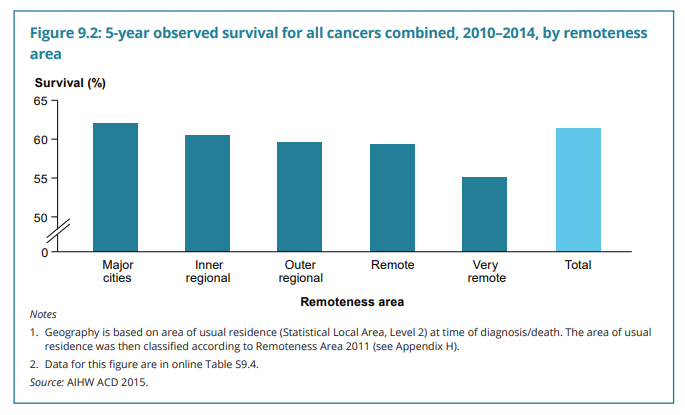
Among the health impacts are a shorter life expectancy, higher mortality, lower cancer survival rates and a higher burden of disease overall. The five-year relative survival rate for all cancers among Indigenous Australians has increased by 3% between 2006 and 2014 to reach 50%, but the gap has been widening; for non-indigenous Australians, the five-year relative survival rate for all cancers increased by 7% to 65% during the same period. The gap in age-standard mortality rates was even wider.
Despite a number of initiatives aimed at improving indigenous health, such as the National Agreement on Closing the Gap, having launched since 2014, inequalities remain. There is a need to encourage screening participation and to provide timely access to diagnostic procedures for all Indigenous Australians to support an improvement in cancer survival rates.
Screening for cancer
AIHW data on participation in our three national cancer screening programs show that uptake varies by remoteness, by socioeconomic group, by indigenous status, as well as by cultural and linguistical background.
Participation is highest in inner regional and outer regional areas for both BreastScreen and bowel screening, and highest in major cities and inner regional areas for cervical screening. For all cancer screening programs, participation is lowest among the most disadvantaged socioeconomic groups.
The largest difference in participation is by indigenous status. There is a far lower uptake for Indigenous Australians when it comes to BreastScreen and bowel screening than for non-Indigenous Australians, with participation also lower among those who speak a language other than English at home. National data for cervical screening is unfortunately not available.
Australia’s national screening programmes play a critical role in detecting common cancers, and it is concerning that participation among remote communities is low. To close the gaps in terms of cancer outcomes and life expectancy, engaging with these groups and encouraging people to test will be essential.
One issue affecting participation rates is that the age structure of the indigenous population is significantly younger than that of non-Indigenous Australians. However, multiple interrelated factors contribute to poorer access and lower uptake of health services in general among this population group.
Diagnostic testing
Usage of further diagnostic tests such as scans and endoscopies is also lower among Indigenous Australians, with timely access to such tests also limited in some cases. One of the major differentiators here is location – or specifically, remoteness.
The Australian Commission on Safety and Quality in Health Care recently investigated rates of repeat colonoscopies and gastroscopies among the Australian population. The results were published in the Fourth Australian Atlas of Healthcare Variation and show that people in metropolitan areas, particularly those with a high socioeconomic status, are tested at higher rates – in some cases too frequently – while people in rural, remote or socioeconomically disadvantaged areas are not being tested at a sufficient rate.
The differences were wide; the rate in areas with the highest use was almost 20 times the rate in areas with the lowest uptake. The data also highlights differences between states and territories, with a rate of 596 repeat colonoscopies per 100,000 people in Queensland, compared with 191 in the Northern Territory.
Access barriers
From an infrastructure perspective, challenges when attempting to improve access to advanced health services include the geographical spread of the population in remote areas, low population density, limited existing infrastructure, limited availability of qualified staff locally and higher costs of delivering rural and remote healthcare services in general.
Evidence has shown that for Aboriginal Australians and Torres Strait Islanders, barriers to accessing health care also include discrimination, cultural differences, distances between the home and the healthcare settings and out-of-pocket healthcare costs. There is also an unmet need for information specifically aimed at Indigenous Australians regarding scans and endoscopy procedures.
Workforce distribution is described in the Atlas as a reason for the low rates of colonoscopy in the rural and remote parts of the country and in areas of socioeconomic disadvantage. While large public teaching hospitals in metropolitan areas serve larger populations and may have limited resources and longer waiting lists, attracting qualified staff may present a significant issue in rural and remote areas.
The development of remote medical consultations and new methods for screening that involve samples taken at home by the patient are helping to reduce the impact of some of the barriers. But if the initial test shows signs of suspected cancer, further diagnostic tests, such as a scan or a colonoscopy, will often be required. An opportunity exists to bring these services closer to patients and make them more accessible and more convenient for all Australians – even those living in more remote locations.
Bringing diagnostics to the patient
One way to do this is to use specialist mobile healthcare facilities. Mobile and modular imaging and endoscopy facilities, such as those provided by Q-bital Healthcare Solutions, can be set up within a short space of time as integral parts of the local health system at a GP surgery, a community hospital, a dental practice or other health related site – either for a fixed time period or in the longer term.
New diagnostic equipment such as scanners and endoscopes is costly, and the usage of any new facility will need to be maximised. For practical and financial reasons, there is a limit to the number of locations that can house an MRI scanner or an endoscopy facility, meaning many patients need to travel some distance to a central location. Instead, a mobile, fully-equipped, mobile diagnostic facility, which is relatively easy to move, could be used on rotation between different locations.
Alternatively, mobile and modular units can be combined to create a stand-alone fixed diagnostic hub in almost any layout, containing patient waiting areas, consultation rooms, scanning and procedure rooms, all specialist equipment, recovery bays, and staff and patient facilities.
Flexible healthcare infrastructure provides a low-risk and less capital intensive solution for increasing access to services. The operational risk to providers is also low, since maintenance and repair is taken care of by the supplier of the facility. Using a collaborative approach brings further benefits and allows the cost of contracting, staffing and equipping the facility, as well as its benefits, to be shared between health providers.
Addressing a specific need
Even where physical access to health services is not limited, the uptake of screening and diagnostic testing services is lower among Aboriginal and Torres Strait Islanders, and there is a need to offer the right services in a way that meets the group’s specific needs.
A holistic approach and a recognition of the cultural values and traditions of indigenous communities are considered key to building trust in the health service, according to the National Safety and Quality Health Service (NSQHS). Strategies to achieve this can include flexible service delivery, so that the patient does not have to attend a hospital or travel long distances, the presence of Indigenous Australian staff at the facility and signs in relevant languages. The fact that the Aboriginal and Torres Strait Islander healthcare work force has declined over time is a concern.
To encourage patients to attend diagnostic appointments, easy to access, targeted information about the procedure may be required for reassurance. At Prince Charles Hospital in Brisbane, for example, medical teams have created a patient education platform, which includes a welcome video aimed at Aboriginal and Torres Strait Islanders that are due to have a colonoscopy. The aim is to reassure unfamiliar patients and help them understand the procedure, and how to best prepare for it.
As well as about the procedure itself, there is also a need to communicate around prevention and the measures people can take to reduce their risk of getting cancer. Around 50% of bowel cancers in Australia are estimated to be due to lifestyle factors, and lung cancer, often caused by smoking, is the leading cause of cancer-related deaths for Aboriginal and Torres Strait Islander people.
Early diagnosis saves lives
Australia is a vibrant, multicultural society; and ensuring equitable access for all its residents, regardless of their cultural background or geographical location, should be a key priority. The level of access and uptake among Indigenous Australians will depend on the success of various government programmes aimed at improving them through a combination of measures.
In some states, significant progress has been made in recent years, and it is encouraging that as part of its commitment to invest $6.7 million to support and improve outcomes for all Australians affected by cancer, the Australian Government has said it will invest in national leadership in Aboriginal and Torres Strait Islander cancer control with the aim of helping to reduce the health gap.
While investing in permanent high-end health infrastructure in each remote location across the country, there is evidence of a very real need to improve both access to, and uptake of, diagnostic services in those areas specifically. A diagnostic hub using flexible healthcare infrastructure, which can be repurposed or moved between locations according to demand, could be a practical solution to a problem that has befuddled governments for decades.
In addition to improving patients’ experiences, increasing access to services locally could drive uptake for diagnostic procedures. The use of flexible healthcare infrastructure, as well as service offers and communication programmes designed specifically with the needs of Aboriginal and Torres Strait Islander people in mind, will play a key role in improving access to diagnostic services for all – for years to come.
For more information about the flexible healthcare facilities offered by Q-bital Healthcare Solutions, please visit the website at www.q-bital.com




